


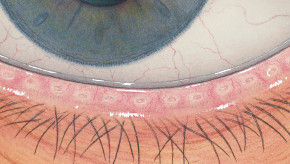


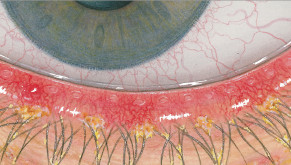

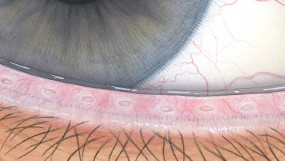
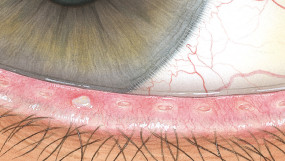
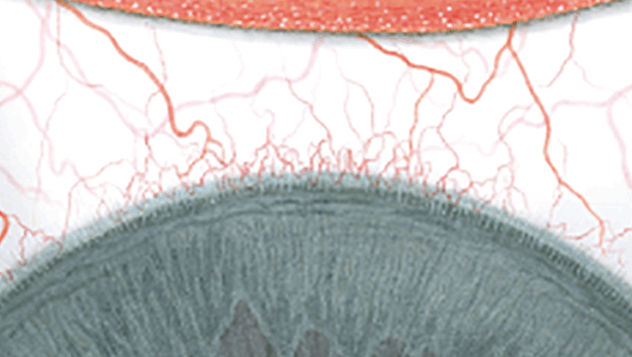
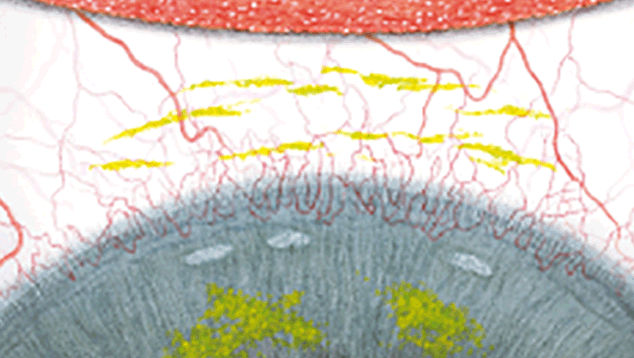
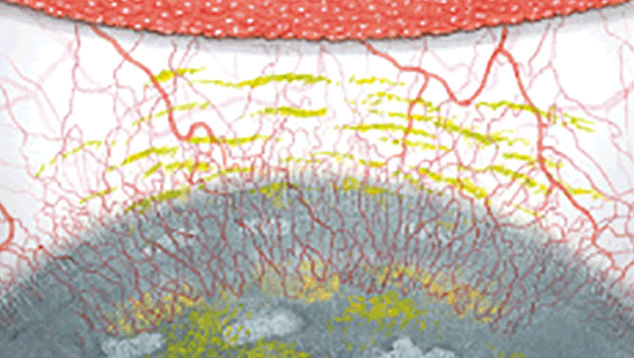
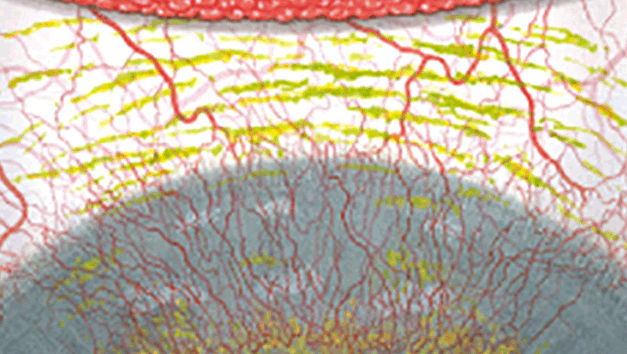
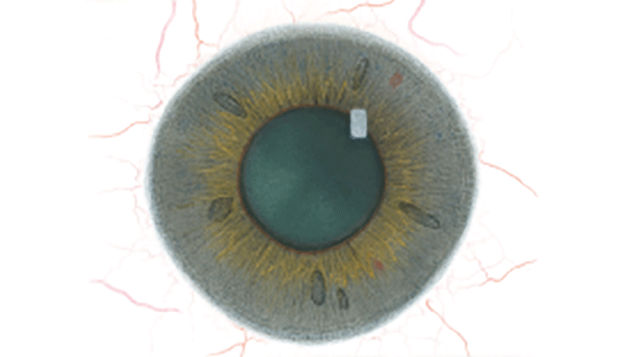
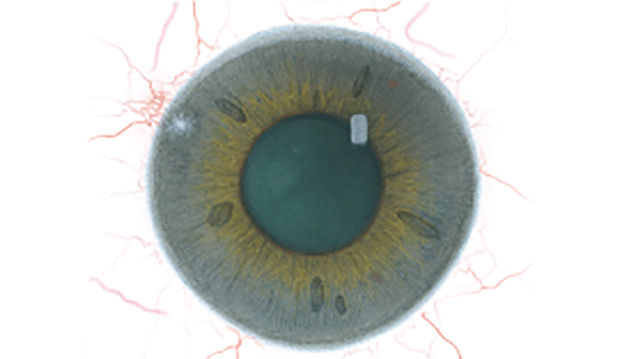
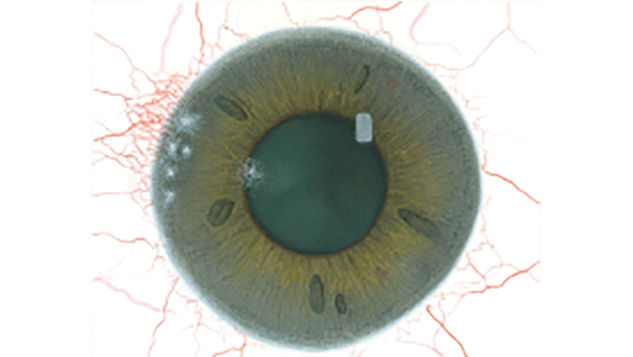
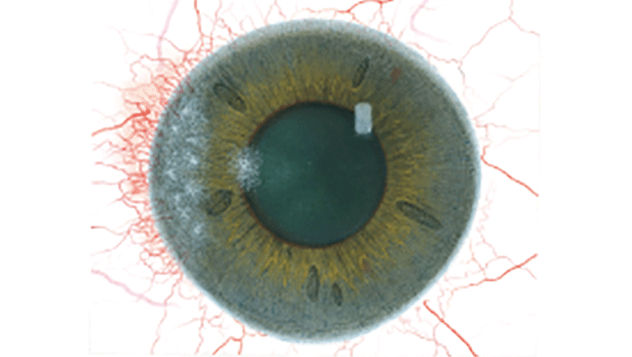
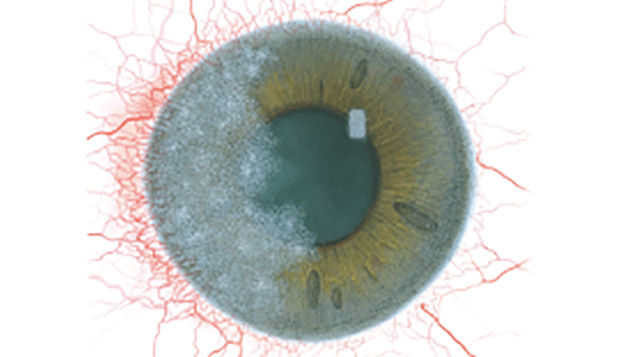
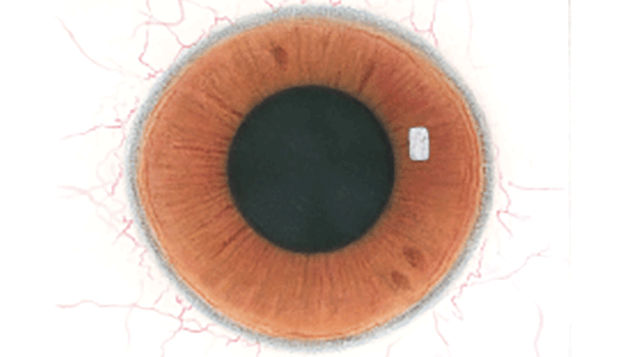

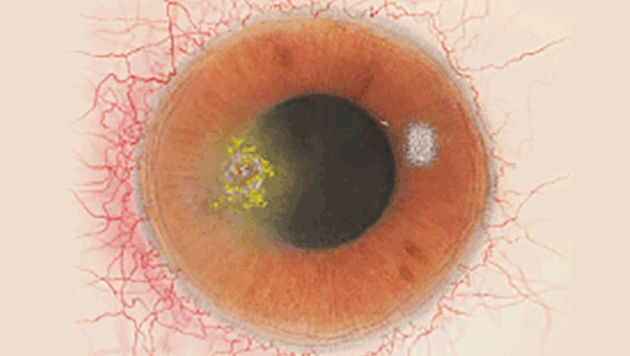
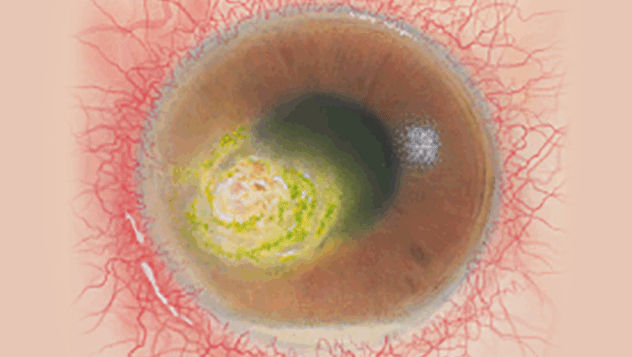















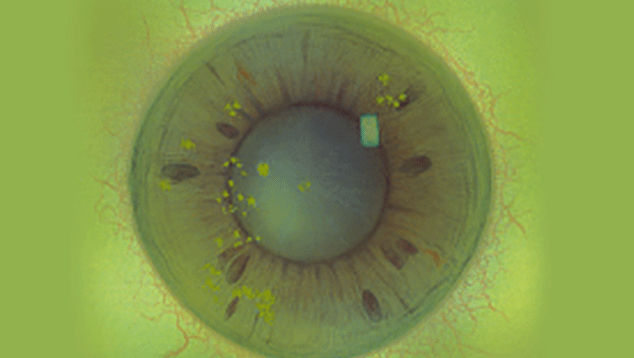
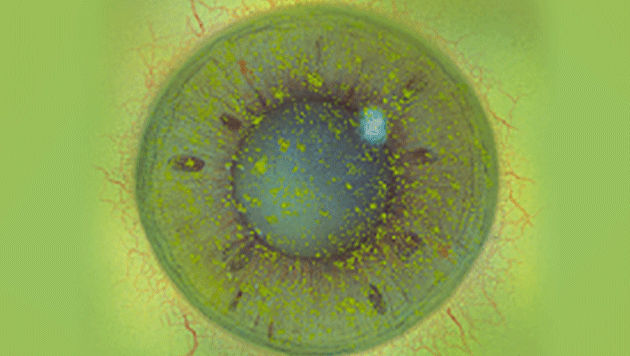
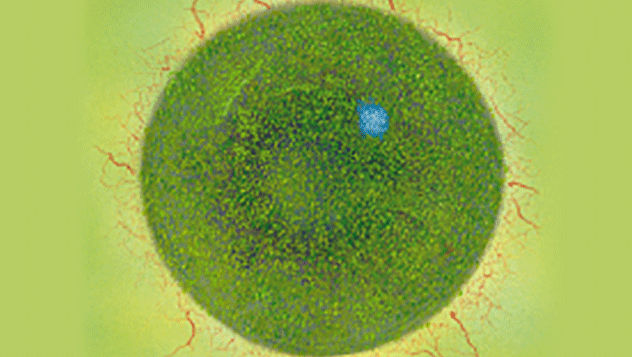


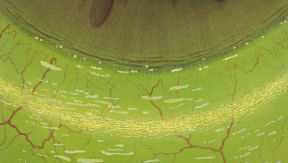


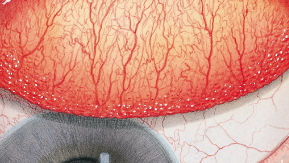



The Efron Grading Scales* provide a convenient clinical reference for eye care professionals.
On a scale of 0 to 4, it describes the severity of the following anterior ocular complications that can occur from contact lens wear.
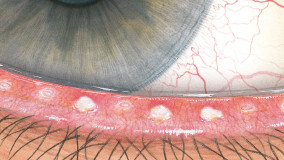
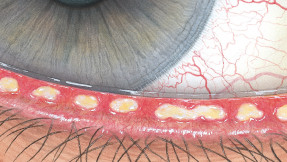
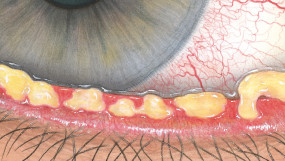
- Blepharitis
- Meibomian gland dysfunction
- Superior limbic keratoconjunctivitis
- Corneal infiltrates
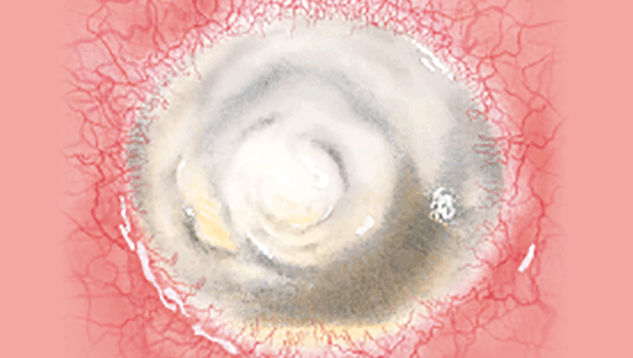
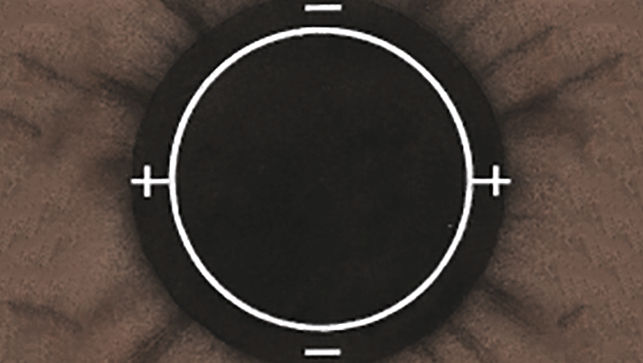
- Corneal ulcer
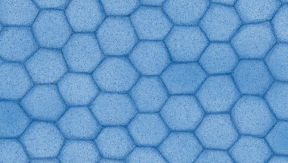
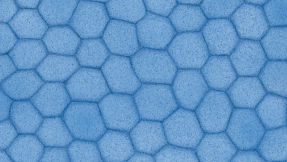
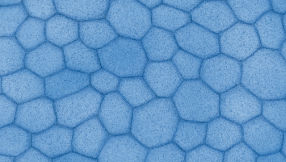
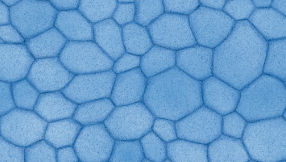
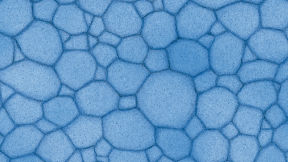
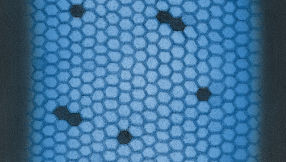
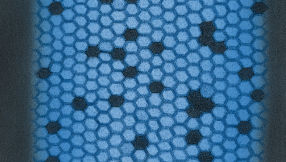
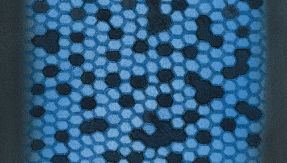
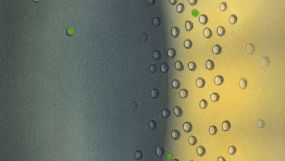
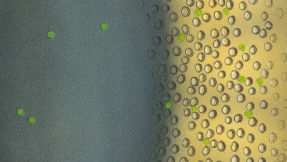
- Endothelial polymegethism
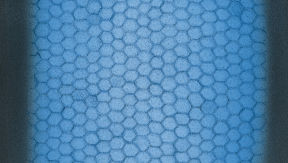
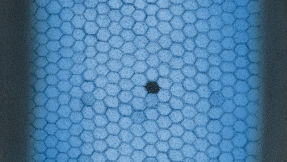
- Endothelial blebs
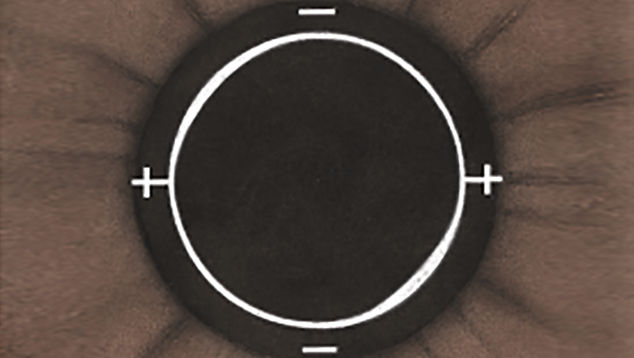
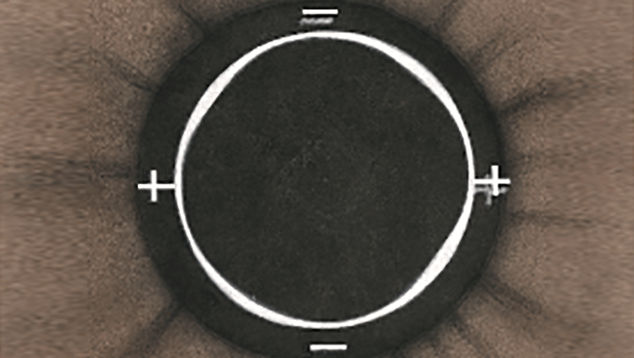
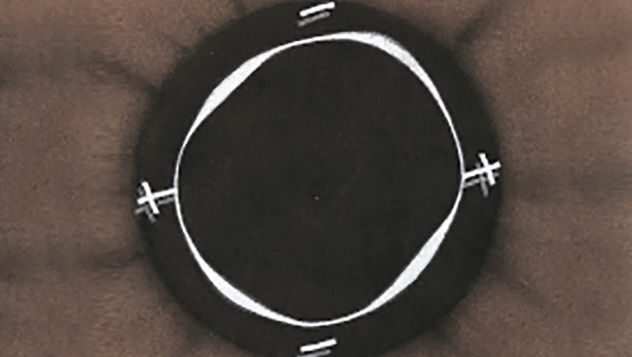
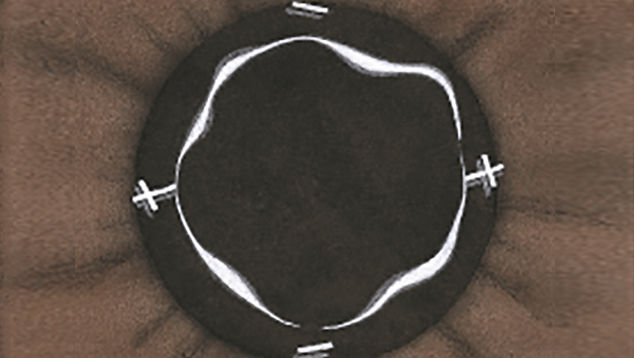
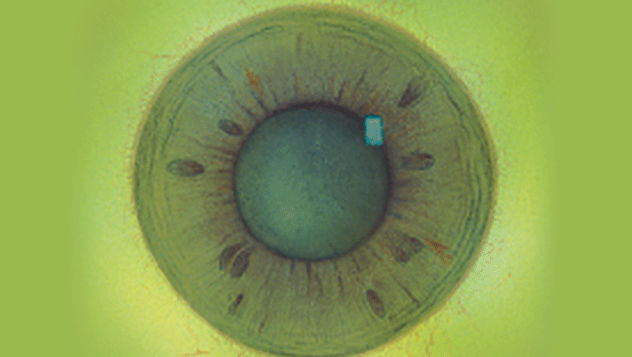
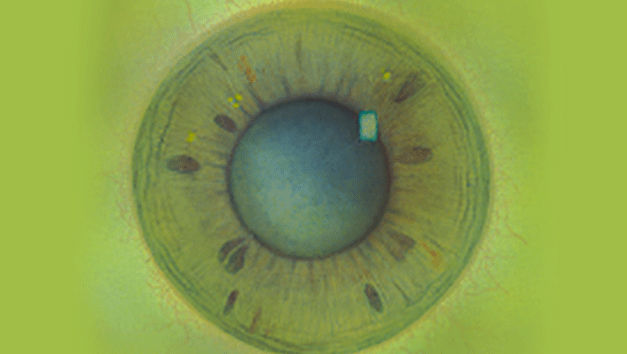
- Corneal distortion
- Conjunctival redness
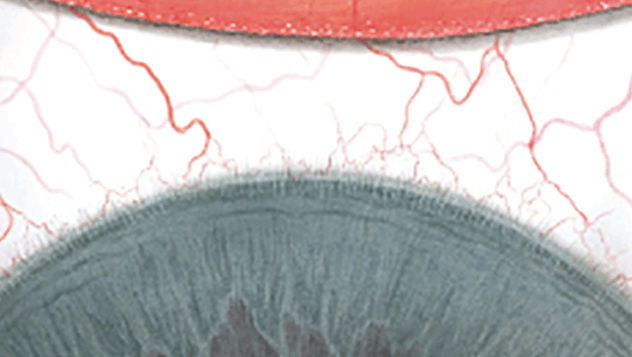
- Limbal redness
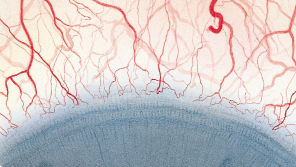
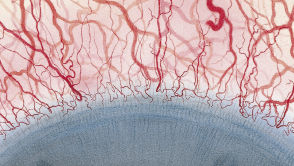
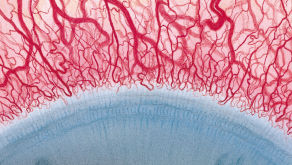
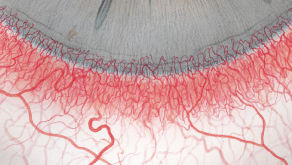
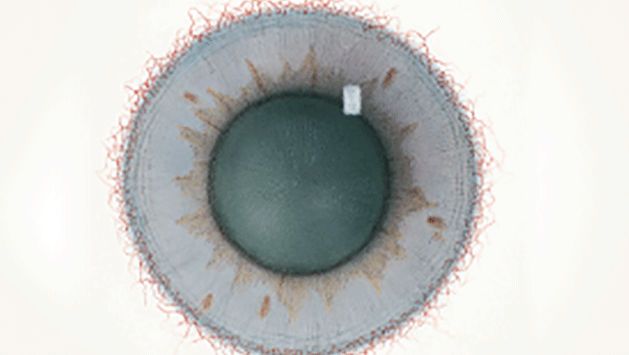
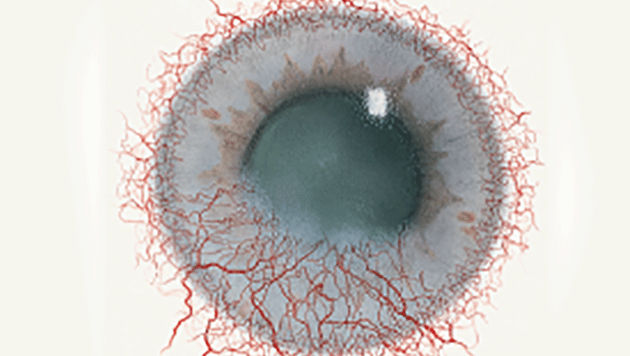
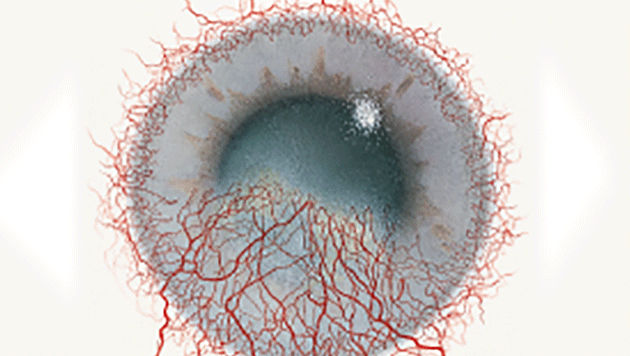
- Corneal neovascularisation
- Epithelial microcysts
- Corneal oedema
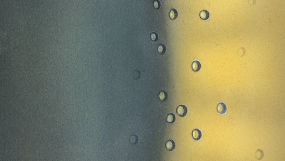
- Corneal staining
- Conjunctival staining
- Papillary conjunctivitis
Each condition includes five illustrations. Simply select a number on the scale for the corresponding illustration and visual signs of severity. Select the Info button for symptoms, pathology, treatment options and more.
* The Efron Grading Scales are designed to help eye care practitioners. It is not a substitute for a professional consultation with a qualified eye care practitioner.